The Office of Insurance Regulation requires
the Medical Professional Liability (MPL) form to be submitted by self-insured
medical facilities, insurers providing coverage for such facilities, or
insurers providing coverage for individual practitioners for any claim
resulting from error, omission, or negligence in the performance of the
insured.
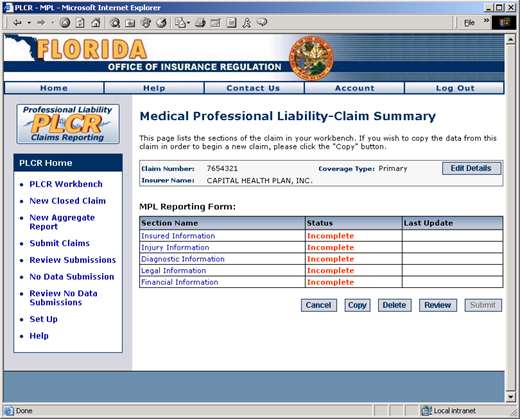
How to Submit an MPL Form
Now that you've completed the initial
steps of creating your new closed claim form, and you understand the
claim summary page you're ready to get
into the details of your MPL form.
On the MPL Claim Summary page below, you'll
notice that the MPL form has five primary sections:
Insured Information
Injury Information
Diagnostic Information
Legal Information
Financial Information
The status of each of these five sections must
be complete in order to submit the form to the Office of Insurance Regulation
for review.
Note: Completing all sections of the MPL form
may take some time. Feel
free to save your data in the current section of the form and return to
other sections as your time permits.
The MPL Claim Summary
Page
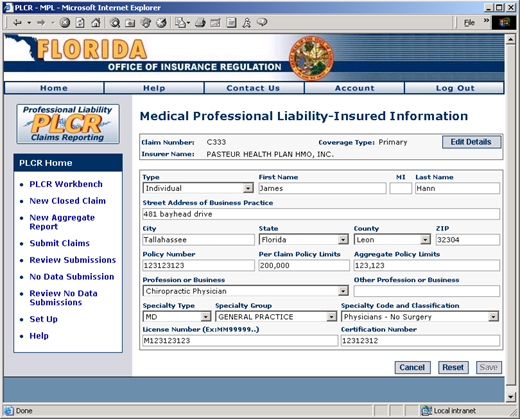
Section 1: Insured Information
The first section of the MPL form provides fields in which you will
enter information about the insured person or entity. Notice
that the if you select an individual, rather than an entity, several additional
fields are required. These
fields include the Specialty Type, Group, and Code and the individual's
licence and certification numbers. The
Insured Information page is displayed below.
The Insured Information
Page
To Edit the Insured Information Page:
Fill in the following list of fields (Fields in
blue apply only if Type: Individual is selected):
Type
Type indicates whether the insured is an individual or entity. Select
Individual or Entity from the drop down box as appropriate.
First Name
The given name of the insured if the Type is Individual.
Middle Initial
The middle initial of the insured if the Type is Individual.
Last Name
The family name/surname of the insured if the Type is Individual.
Entity Name
The name of the insured company if the Type is Entity
Street Address of Business Practice
The street address of the insured's business.
City
The city in which the insured's business is located.
State
The state in which the insured's business is located.
County
The county in which the insured's business is located.
Zip Code
The ZIP/Postal Code address in which the insured's business is located.
Policy Number
The insured's insurance policy number.
Per Claim Policy Limits
The per claim policy limits on the insured's policy.
Aggregate Policy Limits
The aggregate policy limits on the insured's policy.
Profession or Business
The insured's profession or business. If the specific profession or
business is not available in this drop down field, select "Other"
and specify the business in the Other Profession or Business field.
Other Profession or Business
This field is only accessible if "Other" was selected in the
Profession or Business field. This
field is used to type in a profession or business other than those listed
in the Profession or Business drop down field.
Specialty Type
This field indicates the insured's broad area of specialty in the medical
field (e.g., DDS, DO, MD).
Specialty Group
This field further classifies the insured physician's area of expertise.
Note that
for DDS, the only Specialty Group option is Dentistry. There
are several Specialty Group options for DOs and MDs.
Specialty Code
This field further classifies the insured physician's area of expertise.
For example,
a medical doctor (MD) whose Specialty Group is General Practice may have
a Specialty Code of Intensive Care Medicine or Radiation Therapy, etc.
Some physicians
specialties may be limited to only one Specialty Code.
License Number
Also known as the registration number, this is the official number capturing
an attorney or physician's authorization to practice. Note
that the last two-digits of the license number are for the profession
code.
Certification Number
This code indicates that the insured physician is board certified.
Click the Save
button to save your changes and return to the MPL Claim Summary Page.
Clicking
the Reset button will reset all
fields to blank.
Clicking the Cancel button will return you to the
Claim Summary page without saving your changes.
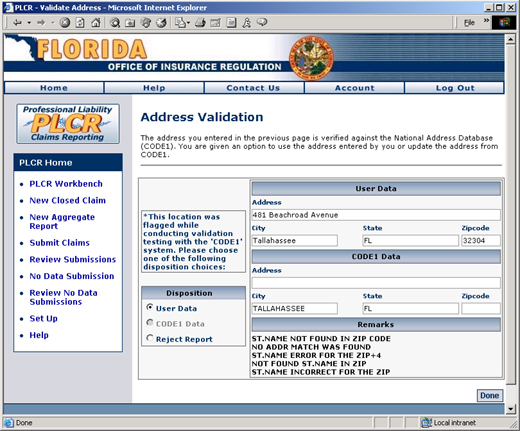
Upon clicking the Save button
all address fields are verified using CODE1 validation. If
the CODE1 validation does not find the address you input into the address
fields, the following Address Validation page will display.
The CODE1 Address Validation
Page
The CODE1 validation page will display the address data you supplied,
CODE1 data that offers a possible known address that is correct, and remarks
regarding the address data.
You may choose to either:
Select "User Data". Selecting
this option will use the address information you supplied, rather than
the CODE1 suggested address.
Select "CODE1 Data". Selecting
this option will use the CODE1 address data found by CODE1 and replace
the address information you supplied.
Select "Reject Report". This
will ignore the CODE1 validation report entirely.
Click the Done button after
making your selection to return to the Insured Information page.
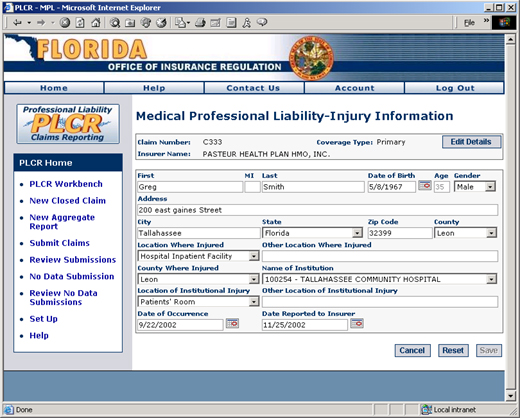
Section 2: Injury Information
The next section of the MPL form provides fields in which you will enter
information about the injured person. The
Injury Information page is displayed below.
The Injury Information
Page
To Edit the Injury Information Page:
Fill in the following list of fields:
First Name
The given name of the injured individual.
Middle Initial
The middle initial of the injured individual.
Last Name
The family name/surname of the injured individual.
Date of Birth
The date of birth of the injured individual. Either type in the date
of the injured individual's birth or select the date of birth from the
calendar to the right of the field.
Age
This is a system calculated field. The
age of the injured individual is determined based on the individual's
birth date and the date of the individual's injury. This
is not the individual's current age, but his/her age at the time of the
injury.
Gender
The sex of the injured individual.
Street Address of Injured Party
The street address of the injured individual's residence.
City
The city in which the injured individual resides.
State
The state in which the injured individual resides.
County
The county in which the injured individual resides.
Zip Code
The ZIP/Postal Code address in which the injured individual resides.
Location Where Injured
The geographical location where the individual was injured. This does not refer to the location of bodily
injury (e.g., spleen, uvula, etc.), but the geographical location where
the patient sustained the injury (e.g., emergency room, nursing home,
etc.).
Other Location Where Injured
If the geographical location of the injured individual is not present
in the drop down field "Location Where Injured", select "Other
Location" and type the name of the location in this field.
County Where Injured
The county where the individual sustained the reported injury. This
is not the injured individual's
county of residence.
Name of Institution
The name of the institution in which the individual was injured (i.e.,
the name of the hospital, nursing home, etc.).
Location of Institutional Injury
The geographical location where the individual was injured within the
institution (e.g., recovery room, critical care unit, etc.).
Other Location of Institutional Injury
If the geographical location of the injured individual is not present
in the drop down field "Location Where Injured", select "Other
Location" and type the name of the location in this field.
Date of Occurrence
The date on which the injury occurred.
Date Reported to Insurer
The date on which the injury was reported to the insurer.
Click the Save
button to save your changes and return to the MPL Claim Summary Page.
Clicking
the Reset button will reset all
fields to blank.
Clicking the Cancel button will return you to the
Claim Summary page without saving your changes.
Upon clicking the Save
button all address fields are verified using CODE1 validation. If CODE1
cannot validate the address information you supplied, the CODE1 Address
Validation page will display. This
page lists the address data you supplied, CODE1 data that offers a possible
known address that is correct, and remarks regarding the address data.
Choose
to accept or reject the CODE1 suggestion as described above and click
the Done button to return to the
Injury Information page.
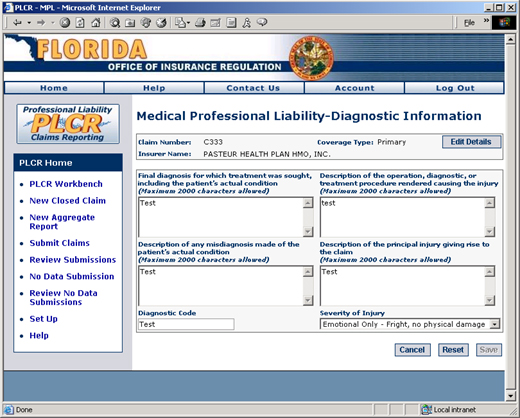
Section 3: Diagnostic Information
This section of the MPL form allows you to enter diagnostic information
related to the injured individual.
The Diagnostic Information Page
To Edit the Diagnostic Information Page:
Fill in the following list of fields:
Final Diagnosis
The final diagnosis for which treatment was sought, including the patient's
actual condition. This
is a free form text box to capture any necessary description up to 2000
characters in length.
Description of Procedure Resulting in Injury
The description of the operation, diagnostic, or treatment procedure
rendered causing the injury. This is a free form text box to capture any
necessary description up to 2000 characters in length.
Description of any Misdiagnosis
The description of any misdiagnosis made of the patient's actual condition.
This is
a free form text box to capture any necessary description up to 2000 characters
in length.
Diagnostic Code
This optional field captures the diagnostic code, if provided.
Description of Injury
The description of the principal injury giving rise to the claim. This
is a free form text box to capture any necessary description up to 2000
characters in length.
Severity of Injury
One of several types of injury severities may be chosen from this drop
down list (e.g., Permanent: Death, Emotional Only, etc.).
Click the Save
button to save your changes and return to the MPL Claim Summary Page.
Clicking
the Reset button will reset all
fields to blank.
Clicking the Cancel button will return you to the
Claim Summary page without saving your changes.
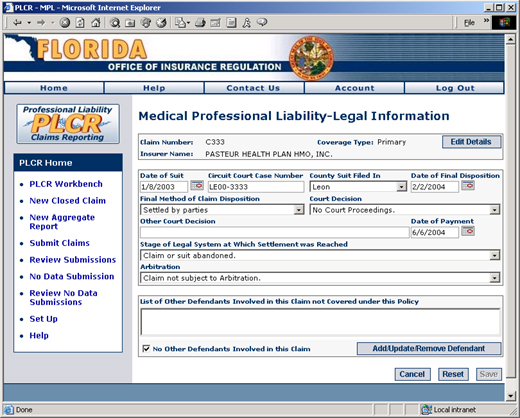
Section 4: Legal Information
Next is the Legal Information section of the MPL form. In
this form you'll fill out information pertaining to the legal action taken
on the medical liability claim. The
Legal Information page is displayed below.
The Legal Information Page
To Edit the Legal Information Page:
Fill in the following list of fields:
Date of Suit
The date the lawsuit of the injured individual was filed against the
insured physician.
Circuit Court Case Number
The circuit court case number assigned to the lawsuit.
County Suit Filed In
The county in which the lawsuit was officially filed.
Date of Final Disposition
The date of the final outcome of the lawsuit (i.e., date of the settlement
or court verdict, etc.).
Final Method of Claim Disposition
The method that resolved the lawsuit (e.g., settled by parties, disposed
of by court, etc.).
Court Decision
The final decision of the court on the lawsuit, if the lawsuit was not
resolved out of court. If
the lawsuit was resolved out of court, select "No Court Proceedings".
Other Court Decision
If the Court Decision rendered does not appear in the drop down list
of Court Decision options, select "Other" from the list of court
decisions and type in the type of court decision.
Date of Final Payment
Enter the date on which the malpractice claim was paid by the insurer,
if a verdict rendered payment necessary. If
no payment was made, leave this field blank.
Stage of Legal System at Which Settlement was Reached
At what point in the legal process was the lawsuit resolved (i.e., after
arbitration, after court verdict, etc.).
Arbitration
Describes the result of the arbitration used to settle the case, if
any.
List of Other Defendants
This is an area where you may add other defendants involved in the case
that are not covered under this policy. If
there are no other defendants, be sure click the checkbox next to the
text "No Other Defendants Involved in this Claim". See step
3 below for more information.
Click the Save
button to save your changes and return to the MPL Claim Summary Page.
Clicking
the Reset button will reset all
fields to blank.
Clicking the Cancel button will return you to the
Claim Summary page without saving your changes.
If you need to add additional defendants involved
in the case that are not covered under this policy or update the list
of defendants, click the Add/Update/Remove
Defendant button. The
Other Defendant Information page will display. If
you do not need to add or update additional defendants, proceed to step
6.
The Other Defendant Information
Page
To Add a Defendant:
Select Individual or Entity from the Type
drop down list.
Enter the name of the entity or individual.
Enter the license number of the entity
or individual.
Click the Add
button. You will notice the name of the entity or individual you added
will appear in the Defendants Involved in this Claim box.
To Remove a Defendant:
Select the individual or entity from the
Other Defendants Involved in this Claim box.
Click the Remove
button. The
defendant will be deleted.
To Update a Defendant:
Select the individual or entity from the
Defendants Involved in this Claim box.
Alter the name of the individual or entity
as appropriate.
Alter the license number as appropriate.
Click the Update
button to finalize the change.
When you are finished updating defendant information,
click the Done button. This
will return you to the Legal Information page.
Click the Save
button to save your changes and return to the MPL Claim Summary Page.
Clicking
the Reset button will reset all
fields to blank.
Clicking the Cancel button will return you to the
Claim Summary page without saving your changes.
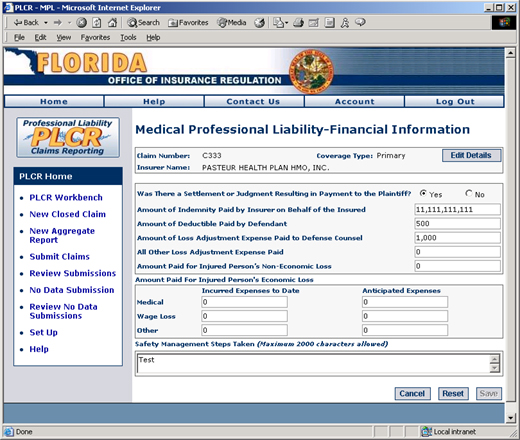
Section 5: Financial Information
The last section of the MPL form you'll need to fill out is the Financial
Information section. This
section captures the monetary values paid to the plaintiff, if any, as
well as costs incurred by the defendant. The
Financial Information page is displayed below.
The Financial Information Page
To Edit the Financial Information Page:
Fill in the following list of fields:
Plaintiff Payment Indicator
Click the radio button next to Yes or No to indicate whether there was
a settlement or judgment resulting in payment to the plaintiff.
Indemnity Paid by Insurer
If the plaintiff received payment as a result of the settlement or judgment,
list the amount of the indemnity paid by the insurer on behalf of the
insured individual.
Deductible Paid by Defendant
List the amount of the deductible paid by the defendant.
Defense Council Expense
List the amount of loss adjustment expense paid to the defense council.
Other Expenses
List all other loss adjustment expenses paid.
Non-Economic Loss Paid
If the plaintiff received payment as a result of the settlement or judgment,
list the amount paid for the injured person's non-economic loss.
Incurred Economic Loss Expenses
List all currently incurred economic loss expenses associated with the
incidence of medical malpractice; including medical, wage loss, and other
expenses.
Anticipated Economic Loss Expenses
List all anticipated economic loss expenses associated with the incidence
of medical malpractice; including medical, wage loss, and other expenses.
Safety Management
List any safety management steps that were taken as a result of this
incident of medical malpractice, if any were necessary.
Click the Save
button to save your changes and return to the MPL Claim Summary Page.
Clicking
the Reset button will reset all
fields to blank.
Clicking the Cancel button will return you to the
Claim Summary page without saving your changes.



.jpg)